Heart valve diseases have always been a major challenge. This is true for both the medical community and patients.
Have you ever suffered from shortness of breath? Or chest pain? Or sudden fatigue without a clear reason? The cause might be aortic stenosis.
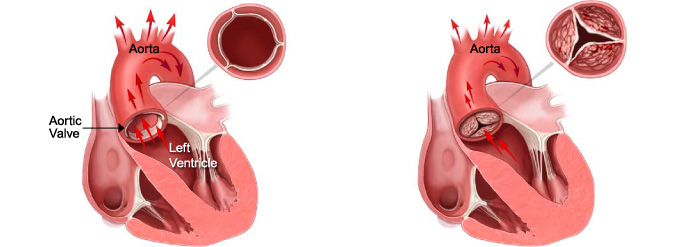
This is a condition where it becomes harder for blood to pass from the left ventricle to the main artery.
In advanced cases, to avoid the risks of open surgery, Transcatheter Aortic Valve Replacement (TAVR) has become an effective non-surgical option.
Leading hospitals worldwide, like Liva Hospital in Turkey, offer the latest TAVR techniques.
We have a team of highly experienced cardiologists and cardiac surgeons. This ensures the best available treatment options for patients.
Heart Valve Diseases and Catheter Intervention
The heart is the body’s main pump.
Its efficiency depends on the proper functioning of its four valves: the aortic valve, the mitral valve, the pulmonary valve, and the tricuspid valve.
These valves open and close in precise synchronization. This ensures blood flows in the correct direction. When valves malfunction, they negatively affect heart function.
Historically, open heart valve replacement surgery was the only effective treatment.
However, this is a major surgery. It requires a chest incision. And connecting the patient to an artificial heart-lung machine.
This exposes patients to high risks of complications and prolonged recovery. Especially the elderly and those with chronic health conditions (like lung disease, kidney disease, or diabetes).
Transcatheter Heart Valve Replacement (THVR) techniques are revolutionary. TAVR for aortic stenosis is a leading example.
It offers a non-surgical alternative for patients considered high-risk or ineligible for open-heart surgery.
Valve diseases are mainly classified into two types:
- Valve Stenosis: This happens when valve leaflets become thick or stiff. They fail to open completely. This hinders blood flow through the valve. The most common example is aortic stenosis. Here, the aortic valve, which regulates blood flow from the left ventricle to the aorta, becomes narrow.
- Valve Regurgitation / Insufficiency: This occurs when valve leaflets don’t close tightly. This leads to blood leaking backward with each heartbeat. It forces the heart to work harder.
Indications for Transcatheter Heart Valve Replacement (THVR)
The decision to perform THVR is made after a precise and comprehensive evaluation.
This is done by a multidisciplinary team known as the “Heart Team.” It includes cardiac surgeons, cardiologists, cardiac imaging specialists, and anesthesiologists.
The team assesses the patient’s general health, the severity of valve disease, and the potential risks of each treatment option. There are many reasons why doctors propose THVR, including:
- Severe Symptomatic Aortic Stenosis: Especially for patients considered at intermediate to high risk or ineligible for open surgery due to advanced age or other co-existing conditions.
- Certain Cases of Mitral Regurgitation using Transcatheter Mitral Valve Repair/Replacement (TMVR): Although less common than TAVR, techniques like MitraClip are used to treat severe mitral regurgitation in patients ineligible for surgery.
- Deterioration of Previously Surgically Implanted Artificial Valves: THVR can be used to implant a new valve inside a previously damaged artificial valve (Valve-in-Valve).
Types of Artificial Heart Valves and Techniques
Advances in artificial valve design and delivery techniques have enabled transcatheter valve replacement procedures.
The valves used in these procedures are often made from biological materials (like animal tissues). They are mounted on a foldable metal frame.
- Valves Used in TAVR (Aortic Valve):
- Self-Expanding Valves: These valves are designed to expand automatically once released from the delivery system. This is driven by the shape-memory properties of the materials (like Nitinol). These valves are flexible and adapt to the shape of the aortic artery.
- Balloon-Expandable Valves: These valves are mounted on a balloon. The balloon is inflated once the valve is correctly positioned. This opens the valve and secures it in the natural aortic valve annulus.
- Valves with Additional Features: Some modern valves offer features to improve performance and reduce complications. These include “shoulders” or “bands” for better stabilization, or coatings to reduce valve calcification.
- Bioprosthetic Valves: All TAVR valves are bioprosthetic (from animal tissues). This means they don’t require lifelong blood thinners (unlike mechanical valves). However, their lifespan is limited (usually 10-15 years or more) compared to mechanical valves.
- Techniques Used in TMVR (Mitral Valve):
- Transcatheter Mitral Valve Repair (TMVr): One of the most common is the MitraClip device. This device does not fully replace the valve. Instead, it’s used to secure the mitral valve leaflets together to reduce regurgitation.
This procedure is less invasive. It’s often the first choice for patients with severe mitral regurgitation who are not deemed eligible for open surgery.
- Transcatheter Mitral Valve Replacement (TMVR): This technique is more complex. It involves implanting a new artificial valve inside the damaged native mitral valve. This technique is still in advanced stages of development and research. It’s used in very specific cases.
- Transcatheter Mitral Valve Repair (TMVr): One of the most common is the MitraClip device. This device does not fully replace the valve. Instead, it’s used to secure the mitral valve leaflets together to reduce regurgitation.
How is Transcatheter Heart Valve Replacement Performed?
Transcatheter Heart Valve Replacement (specifically TAVR) is a highly precise procedure.
It requires the expertise of a multidisciplinary team. It also needs the latest technologies in a hybrid cardiac catheterization lab. The procedure is usually performed under general anesthesia or local anesthesia with deep sedation.
- Anesthesia and Access:
- The patient receives appropriate anesthesia.
- The doctor makes a small incision (about 0.5 to 1 cm) at the chosen access site. This is most often the femoral artery in the groin area (Transfemoral Approach). Advanced imaging techniques (like X-ray) guide the catheter.
- A sheath is inserted into the artery. This is used as a safe entry point for introducing instruments.
- Catheter Insertion and Guidance:
- A thin, flexible guidewire is passed through the sheath into the aorta. It is then carefully guided across the damaged native aortic valve into the left ventricle of the heart.
This guidance is assisted by real-time Fluoroscopy and Transesophageal Echocardiography (TEE) to ensure accuracy.
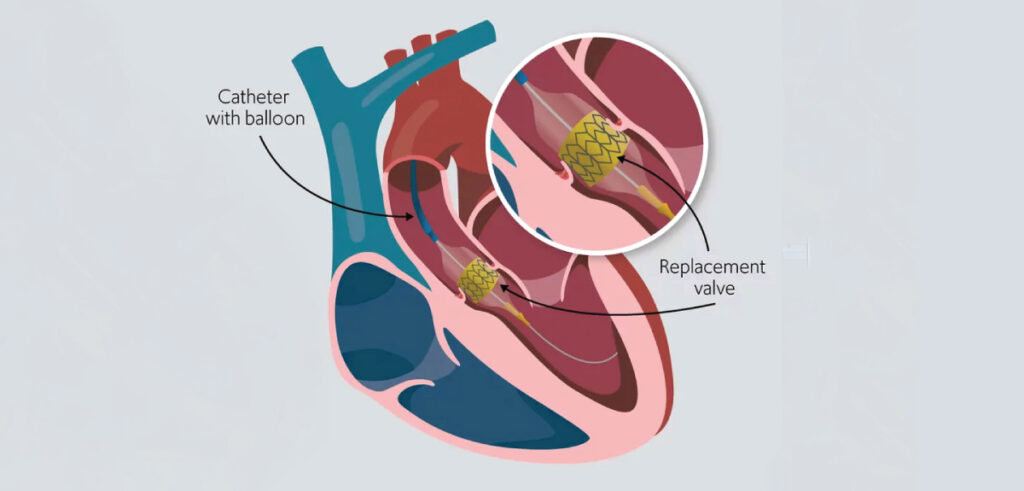
- A specialized delivery catheter carries the new, folded (compressed) valve. It is guided over the guidewire to the old aortic valve’s location.
- A thin, flexible guidewire is passed through the sheath into the aorta. It is then carefully guided across the damaged native aortic valve into the left ventricle of the heart.
- Preparation of the Old Valve (Optional):
- In some cases, especially if the old aortic valve is severely calcified, Balloon Valvuloplasty may be performed first. A balloon catheter is passed and inflated inside the old aortic valve to slightly widen the opening. This prepares it to receive the new valve.
- Implantation of the New Valve:
- When the new, folded valve is positioned correctly inside the old valve (or where the old valve was removed in open surgery), it is released and opened.
- If it’s a self-expanding valve, it expands automatically. If it’s a balloon-expandable valve, a balloon inside the valve is inflated to open it and firmly secure it in the native aortic valve annulus. This part takes only a few seconds.
- The medical team carefully monitors blood flow and the function of the new valve using echocardiography and X-rays.
- Removal of Instruments and Closure of Access Site:
- After confirming the new valve is functioning correctly, all catheters and guidewires are carefully withdrawn.
- The access site in the groin is closed using special closure techniques (like closure sutures) or manual pressure to ensure bleeding stops.
Recovery After Transcatheter Heart Valve Replacement
Since Transcatheter Heart Valve Replacement (specifically TAVR) is much less invasive than open-heart surgery, the recovery period is shorter and more comfortable. This allows most patients to return to their normal lives more quickly.
- Early Stage (In Hospital – A Few Days):
- Intensive Care Unit (ICU) or Cardiac Care Unit: After the procedure, the patient is transferred to the ICU or cardiac care unit for close monitoring of vital signs, heart function, and the access site.
- Rest and Early Mobilization: The patient is asked to rest in bed for several hours after the procedure. However, the patient is encouraged to move and walk short distances with nursing assistance as soon as possible (usually the same day or the next day) to avoid complications and improve circulation.
- Pain Management: Pain is usually mild to moderate. It can be controlled with prescribed pain relievers.
- Nutrition: The patient can start taking liquids and light food as soon as their condition allows.
- Hospital Discharge: In most cases, the patient can be discharged from the hospital within 2 to 5 days after the procedure, once their condition is stable.
- Intermediate Stage (At Home – A Few Weeks):
- Access Site Care: The access site must be kept clean and dry to avoid infection. There might be a small bruise or mild swelling that gradually disappears.
- Physical Activity: It is recommended to gradually increase activity. The patient can resume most light daily activities within a week. Avoid heavy lifting or strenuous activities for several weeks.
- Medications: Adherence to prescribed medications is crucial. Heart medications will be prescribed. The patient may need to take blood thinners (like aspirin and another antiplatelet drug) for a specific period. This prevents blood clot formation on the new valve.
- Cardiac Rehabilitation: Joining a Cardiac Rehabilitation program is highly recommended. This is a supervised program that helps patients regain physical fitness, learn how to manage heart disease risk factors, and improve their overall lifestyle.
- Long-Term Stage (Months and Years):
- Regular Follow-up: Regular follow-up with a cardiologist is essential. This assesses the new valve’s performance. It also monitors heart function. And ensures no complications.
- Adherence to a Healthy Lifestyle: Maintaining a heart-healthy lifestyle is vital. This includes a balanced diet, exercise, quitting smoking, and managing chronic diseases. This is for long-term heart and new valve health.
- Expectations: The majority of patients report significant improvement in symptoms and quality of life after TAVR. This allows them to return to a more active and independent lifestyle.
Potential Risks and Complications
Although Transcatheter Heart Valve Replacement is less invasive than open-heart surgery, it carries some potential risks and complications.
These complications are relatively rare. But it’s important for patients to be aware of them. And to discuss them with their medical team.
- Vascular Access-Related Risks:
- Severe bleeding or bruising: At the access site (often the groin).
- Blood vessel damage: Artery tearing or dissection may occur during catheter insertion.
- Heart and Valve-Related Risks:
- Stroke: Although rare (about 1-5%), stroke can occur. This is if a blood clot or parts of calcification detach from the old valve or blood vessels. And travel to the brain.
- Problems with the heart’s electrical conduction system: The new valve may affect the heart’s natural electrical conduction system. This causes slow heartbeats and requires permanent pacemaker implantation (about 5-20% of cases).
- Paravalvular Leak: The new valve may not seal perfectly with the old valve’s tissues. This causes a small blood leak around the valve. In most cases, the leak is mild and causes no problems. But a large leak may require additional intervention.
- Coronary artery obstruction: In very rare cases, the new valve may cover the openings of the coronary arteries. This affects blood flow to the heart muscle and causes a heart attack.
- Valve or Aortic Rupture: A rare but very serious complication.
- Infection: Risk of infection (infective endocarditis) on the new valve, although rare.
- General Risks:
- Kidney problems: The contrast dye used in X-rays can cause kidney damage. Especially in patients with pre-existing kidney problems.
- Pulmonary Edema: Fluid accumulation in the lungs.
- Death: Although success rates are high, there’s always a small risk of death associated with any major medical procedure.
Conclusion
Transcatheter Heart Valve Replacement (THVR), particularly TAVR, is a remarkable success story in cardiology. It embodies medical innovation that can change millions of lives.
From being an option for patients unable to undergo open-heart surgery, THVR has evolved.
It has become a standard alternative for intermediate to high-risk patients. There is also a promise of opening new avenues for low-risk patients in the future.
This technique not only reduces the risks associated with major surgery. It also accelerates the recovery process. This allows patients to return to their normal lives with a better quality of life.
This achievement would not have been possible without the unique synergy. It is between advanced medical expertise and sophisticated technologies.
This procedure is complex. It requires a highly trained and experienced team.
These procedures are performed in hospitals equipped with the latest technologies, such as Liva Hospital in Turkey. This ensures the highest standards of safety and accuracy.
Frequently Asked Questions
Is Transcatheter Heart Valve Replacement (TAVR) a permanent treatment?
Yes, the new valve implanted in a TAVR procedure is a permanent valve. It aims to function for many years. Most currently used valves are bioprosthetic (made from animal tissue). They are expected to last between 10 to 15 years or more.
Do I need to take blood thinners for life after TAVR?
Usually no. Since most TAVR valves are bioprosthetic, the need for lifelong blood thinners (like warfarin) is rare. However, you may be prescribed an antiplatelet medication (like aspirin or clopidogrel) for a specific period.
How long does recovery take after TAVR?
Since TAVR is a non-surgical procedure, recovery is much faster than open-heart surgery. Most patients can be discharged from the hospital within 2-5 days. They can return to light daily activities within a week or two.
Can TAVR be performed for all types of heart valve problems?
Currently, TAVR is primarily used to treat severe aortic stenosis. There are also techniques used to repair or replace the mitral valve via catheter in selected cases.
What are the alternatives if I am not a candidate for TAVR?
If you are not eligible for TAVR, alternatives may include open-heart aortic valve replacement surgery (if risks are acceptable). Or medical therapy to control symptoms if the condition is mild to moderate or if surgery is not possible.
Can I exercise after TAVR?
Yes, after the recovery period and once your doctor approves, most patients are encouraged to gradually return to exercise and physical activities.